For decades, medical advice for parents was rooted in a philosophy of strict avoidance. Families were told to keep peanuts away from infants, sometimes until age three, to prevent life-threatening allergies. However, as avoidance became the norm, peanut allergy rates in Western nations didn’t just stay steady—they skyrocketed.
Today, we are witnessing a paradigm shift. Groundbreaking research, most notably the LEAP (Learning Early About Peanut Allergy) studies, has turned traditional wisdom on its head. We now know that the immune system needs a “friendly introduction” to peanut proteins during a critical window in infancy. Introducing peanut-containing foods as early as 4 to 6 months of age can provide lasting protection that extends into adolescence.
1. What is a Peanut Allergy?
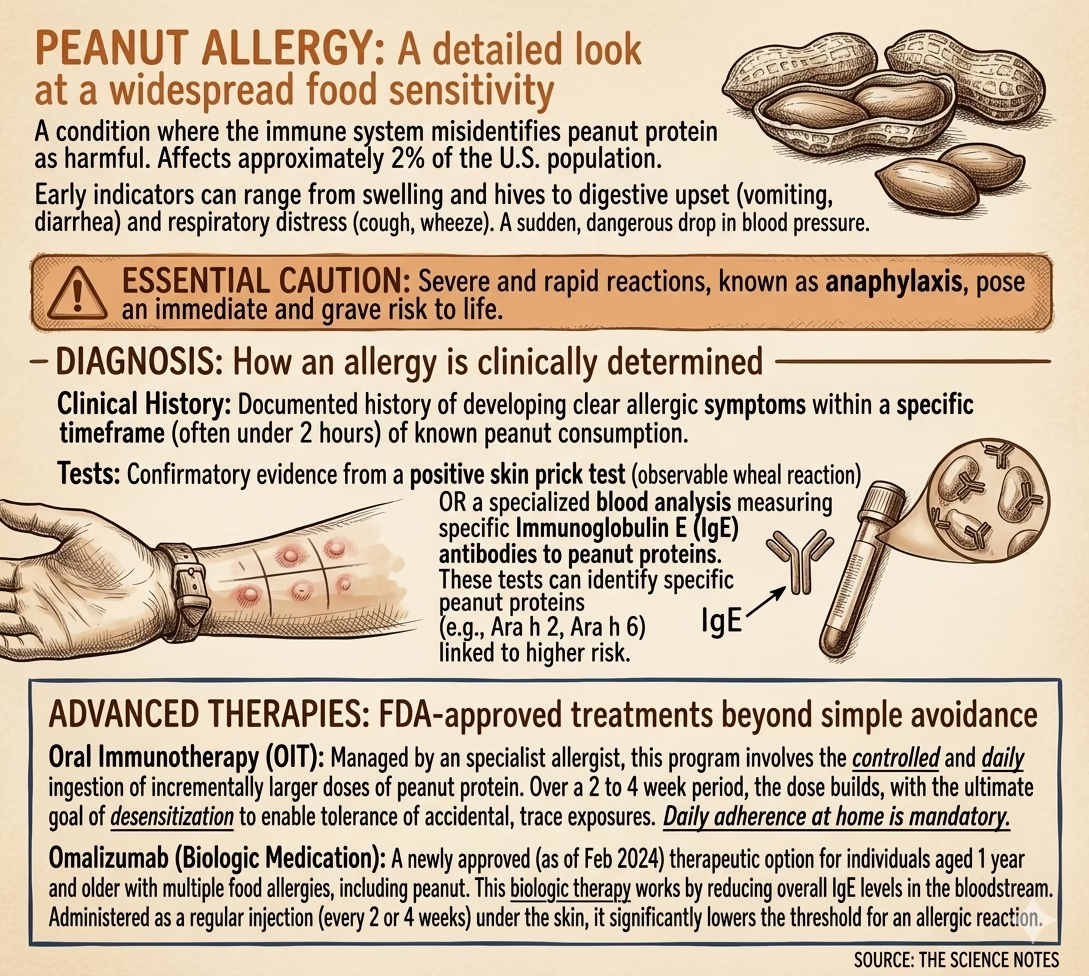
At its core, a peanut allergy is a case of mistaken identity by the immune system. It occurs when the body’s internal defense system reacts to harmless peanut proteins as if they were dangerous pathogens like a virus or bacteria.
The Role of IgE Antibodies
When an individual with a peanut allergy is exposed to the protein, their immune system produces Immunoglobulin E (IgE) antibodies. These antibodies “prime” the body’s mast cells. The next time peanut protein enters the system, these antibodies trigger the release of chemicals, including histamine, which cause physical symptoms.
Symptoms of a Reaction
Symptoms usually develop within 1 to 2 hours of ingestion. Because the immune response is systemic, it affects multiple organs:
Skin: Swelling of the lips/tongue, hives (urticaria), and generalized redness or itching.
Gastrointestinal: Nausea, vomiting, stomach cramps, and diarrhea.
Respiratory: Persistent cough, wheezing, chest tightness, or a “tight” throat.
Cardiovascular: A sudden drop in blood pressure (hypotension), dizziness, or fainting.
The Threat of Anaphylaxis
Anaphylaxis is a severe reaction involving more than one body system (e.g., hives combined with wheezing). While the risk of death is statistically low—approximately 1 in 10 million—its unpredictable nature causes significant psychological stress for families.
2. The Science of Prevention: LEAP to LEAP-Trio
The journey began twenty years ago when researchers noticed that children in countries where peanuts were a dietary staple in infancy had much lower allergy rates.
The LEAP Study (Infancy to Age 5)
Researchers followed 640 “high-risk” infants (those with severe eczema or egg allergies).
The Result: Early introduction reduced the risk of peanut allergy by 81% by age five.
LEAP-On: Is Protection Durable?
Participants from the “consumption” group were asked to avoid peanuts from age 5 to 6. Even after a year of avoidance, the majority remained protected, suggesting the “off-switch” for the allergy was permanent.
LEAP-Trio: Protection into Adolescence
Published in NEJM Evidence (May 2024), this study followed the original participants to age 13.
Early Exposure Group: Only 4.4% developed an allergy.
Avoidance Group: 15.4% developed an allergy.
The Takeaway: Early introduction represents a 71% reduction in adolescent peanut allergies.
3. Diagnosis and Treatment
Diagnosing a peanut allergy is a precise process. It is not enough to have a “positive test”; results must be interpreted by an allergist in the context of symptoms.
Diagnostic Criteria
Skin Prick Test: An allergist pricks a tiny amount of protein into the skin. A raised, red bump (wheal) within 20 minutes indicates the presence of IgE antibodies.
Blood Test (sIgE): Measures the level of specific IgE antibodies in the bloodstream.
Modern Treatment Options
We have moved from “passive avoidance” to “active desensitization.”
Epinephrine (Emergency): The first-line treatment for anaphylaxis. It constricts blood vessels to raise blood pressure and relaxes lung muscles to open airways.
Oral Immunotherapy (OIT): Supervised, gradual ingestion of peanut protein to build tolerance. About 80% of individuals are successfully desensitized this way.
Omalizumab (Biologic): An FDA-approved injection (as of Feb 2024) that “mops up” IgE antibodies before they can trigger a reaction.
4. Practical Guide for Parents
The 2017 NIAID guidelines recommend introducing peanut-containing foods between 4 and 6 months of age.
Assessing Risk
High-Risk: Infants with severe eczema or egg allergy. Consult an allergist before introduction.
Low-to-Moderate Risk: Infants with no or mild eczema. Introduce Peanuts at home once other solids have started.
Safe Introduction Methods
⚠️ Safety Warning: Never give an infant whole peanuts or large chunks of peanut butter. These are major choking and aspiration hazards.
Thinned Peanut Butter: Mix 2 tsp of smooth peanut butter with 2-3 tsp of warm water, breast milk, or formula.
Peanut Puffs: Dissolve puffs (like Bamba) in liquid or offer them whole if the baby is adept at finger foods.
Peanut Flour/Powder: Mix a small amount into a fruit or vegetable puree.
Summary: Key Takeaways
Start Early: 4–6 months is the critical window for protection.
Be Consistent: Regular consumption is more effective than occasional exposure.
Stay Prepared: If you have a preexisting allergy, always carry epinephrine and stay informed on new biologic treatments.
For more evidence-based health guides, visit www.thesciencenotes.com.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult with a healthcare professional regarding your child’s health.
More information: https://www.nih.gov/news-events/nih-research-matters/providing-lasting-protection-peanut-allergy