Enterobiasis, commonly known as pinworm infection, is one of the most frequent parasitic infections worldwide, particularly affecting children. Caused by the small nematode Enterobius vermicularis, this infection can lead to discomfort, sleep disturbances, and, in rare cases, complications in the female genital tract. In this article, we explore the biology, life cycle, clinical features, diagnosis, and prevention strategies of Enterobiasis to provide a comprehensive understanding for students, healthcare professionals, and curious readers.
What is Enterobiasis?
Enterobiasis is an intestinal infection caused by the roundworm Enterobius vermicularis. Belonging to the Phylum Nemathelminthes, Class Nematoda, and Genus Enterobius, the species vermicularis is uniquely adapted to the human gastrointestinal tract. Its common name, “pinworm,” derives from the adult female’s slender, pointed tail, which resembles a pin.
The infection is transmitted primarily through the ingestion of eggs, which can occur by self-inoculation (touching the mouth after scratching the anal area) or through exposure to contaminated surfaces, clothing, or bedding. After ingestion, the eggs hatch in the small intestine, mature into adults, and begin reproducing, completing a lifecycle that can take one to two months or longer.
Habitat and Geographical Distribution
Enterobius vermicularis primarily inhabits the large intestine, particularly the cecum and appendix. Pinworm infection is globally prevalent, with a higher incidence in children due to close contact environments like schools and daycare centers. Household transmission is common because eggs can survive on surfaces and spread easily among family members.
Life Cycle of Enterobius vermicularis
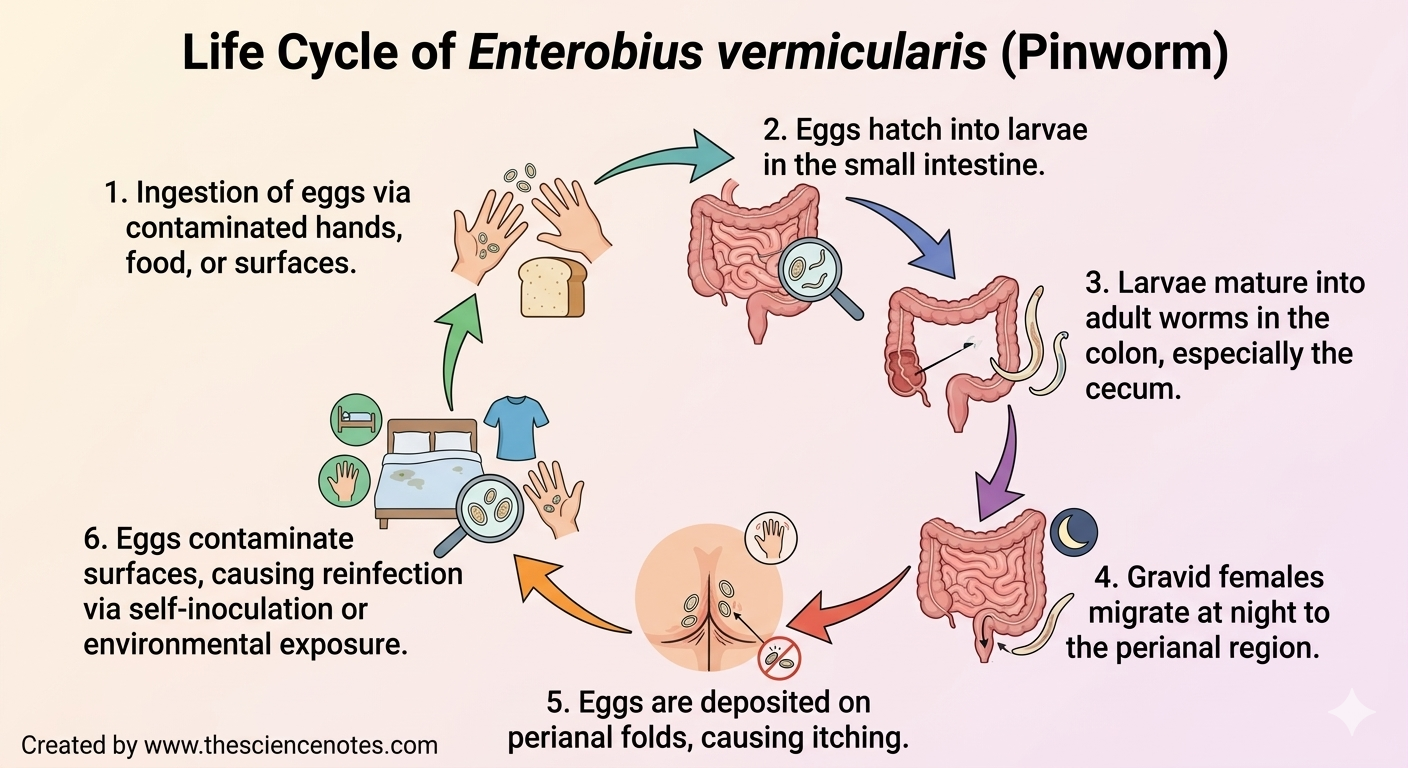
Understanding the life cycle of E. vermicularis is crucial for effective treatment and prevention:
Egg Deposition: Gravid females migrate to the perianal region at night and lay eggs on the skin.
Transmission: Infection occurs through self-inoculation or contact with contaminated surfaces (e.g., bed linens, clothing, toys). Rarely, eggs can become airborne and be inhaled.
Larval Hatching: After ingestion, eggs hatch in the small intestine, releasing larvae.
Adult Maturation: Larvae migrate to the colon, mainly the cecum, where they mature into adults. The adult female measures 8–13 mm, while males are smaller, 2–5 mm.
Reproduction: The adult lifespan is about two months, during which females continue nocturnal egg deposition.
Retroinfection: Occasionally, larvae may re-enter the rectum from the anal skin, perpetuating infection.
Key point: Eggs become infective within 4–6 hours under optimal conditions, emphasizing the importance of hygiene to prevent reinfection.
Clinical Manifestations
Many cases of Enterobiasis are asymptomatic, but common symptoms include:
Perianal pruritus: Intense itching, especially at night, often leading to bacterial superinfection.
Sleep disturbances: Insomnia and restlessness due to itching.
Gastrointestinal issues: Abdominal pain, irritability, anorexia.
Other signs: Teeth grinding (bruxism), bedwetting (enuresis), and in females, vulvovaginitis or pelvic granulomas.
Appendiceal involvement: Larvae are sometimes discovered during appendectomy, mimicking appendicitis.
Recognizing these symptoms early helps prevent complications and reduces household transmission.
Laboratory Diagnosis
Diagnosing Enterobiasis can be straightforward with three commonly used methods:
Direct Observation: Visual inspection of the perianal region 2–3 hours after the infected person falls asleep.
Tape Test: Transparent tape is applied to the perianal area in the morning to collect eggs, which are then examined under a microscope. Repeating this test for three consecutive mornings improves accuracy.
Fingernail Examination: Eggs may accumulate under fingernails due to scratching, and these samples can be examined microscopically.
Early and accurate diagnosis is essential for timely treatment and preventing reinfection within households or institutions.
Treatment Options
Effective medical treatments for pinworm infection include:
Mebendazole
Pyrantel pamoate
Albendazole
In households where multiple members are infected, simultaneous treatment is recommended to prevent ongoing transmission. Healthcare providers may advise repeating treatment after two weeks to target newly hatched worms.
Prevention and Control
Preventing Enterobiasis focuses on personal hygiene, environmental sanitation, and routine household care:
Handwashing: Wash hands with soap and warm water after using the toilet, changing diapers, or before eating.
Bathing: Infected individuals should bathe each morning to remove eggs from the skin.
Nail Hygiene: Keep fingernails short and avoid biting or scratching.
Laundry Management: Frequently change underclothes and bed linens, washing them in hot water followed by a hot dryer to kill eggs. Avoid shaking clothes or bedding to prevent dispersing eggs.
Environmental Cleaning: Clean household surfaces regularly to reduce the risk of transmission.
In institutions such as schools and daycare centers, mass drug administration may be necessary during outbreaks, alongside strict hygiene practices.
Key Takeaways
Enterobiasis is a common parasitic infection, especially among children.
Infection occurs via ingestion of eggs through direct contact or contaminated surfaces.
Typical symptoms include perianal itching, sleep disturbances, and irritability; complications are rare but possible.
Diagnosis can be made through tape tests, fingernail examination, or direct observation.
Treatment is simple with antiparasitic medications, but prevention through hygiene is crucial to stop reinfection.
By understanding the life cycle, symptoms, and preventive strategies of Enterobius vermicularis, individuals and households can effectively control the spread of pinworm infection and protect overall health.