Author: Alisha G C
Abstract
Teclistamab is a first-in-class bispecific antibody targeting B-cell maturation antigen (BCMA) and CD3 that has significantly advanced the treatment of relapsed or refractory multiple myeloma (RRMM). By simultaneously binding malignant plasma cells and cytotoxic T lymphocytes, Teclistamab redirects endogenous T cells to eliminate BCMA-expressing tumor cells through major histocompatibility complex (MHC)–independent immune activation. This mechanism bypasses limitations associated with conventional chemotherapy and antigen-restricted immunotherapies. Clinical trials have demonstrated substantial response rates in heavily pretreated multiple myeloma patients, including individuals refractory to proteasome inhibitors, immunomodulatory drugs, and anti-CD38 monoclonal antibodies. However, therapeutic resistance driven by antigen downregulation, T-cell exhaustion, and tumor microenvironment–mediated immune suppression remains a significant challenge. This review provides an in-depth analysis of Teclistamab’s molecular architecture, immunologic mechanism of action, pharmacokinetics, clinical efficacy, resistance pathways, and emerging strategies designed to enhance therapeutic durability.
Molecular Structure of Teclistamab
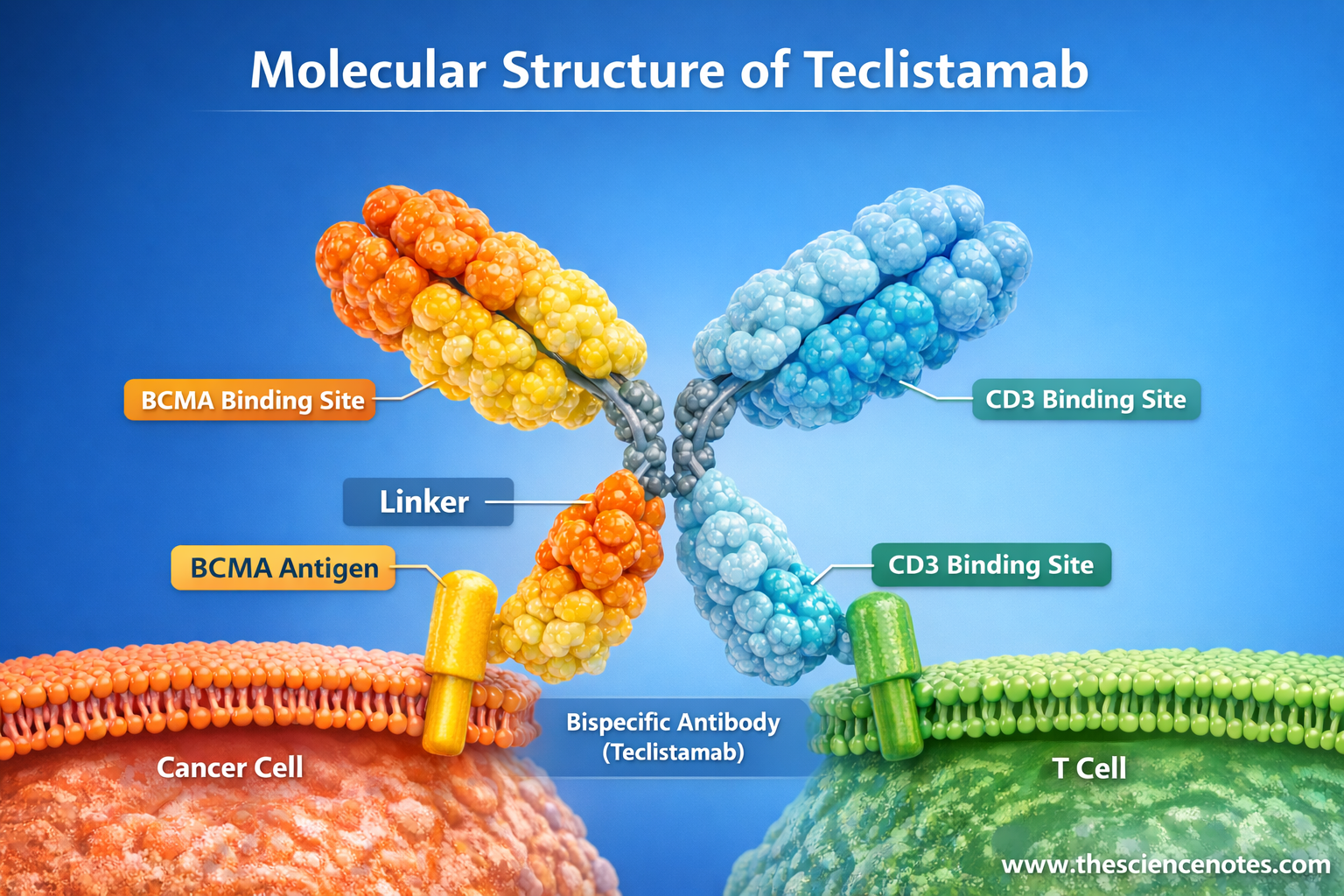
Teclistamab is a humanized bispecific IgG4 monoclonal antibody engineered to simultaneously bind:
B-cell maturation antigen (BCMA) on malignant plasma cells
CD3ε on T lymphocytes
This dual-binding configuration enables direct immune synapse formation between T cells and tumor cells, triggering targeted cytotoxic responses.
Unlike smaller bispecific T-cell engager (BiTE) molecules such as Blinatumomab, Teclistamab retains a modified Fc domain, which improves structural stability and pharmacokinetic properties while minimizing unwanted immune activation.
Key structural characteristics include:
Full-length IgG-based bispecific antibody architecture
Engineered Fc region with reduced Fcγ receptor binding
Enhanced serum half-life compared with Fc-less bispecific antibodies
Capability for subcutaneous administration
This design enables sustained therapeutic exposure while reducing the need for continuous infusion.
BCMA: The Plasma Cell Targeting Domain
B-cell maturation antigen (BCMA, also known as TNFRSF17) is a transmembrane receptor belonging to the tumor necrosis factor receptor (TNFR) superfamily. It is expressed primarily on:
Long-lived plasma cells
Malignant plasma cells in multiple myeloma
BCMA plays a central role in plasma cell survival by binding the ligands:
BAFF (B-cell activating factor)
APRIL (a proliferation-inducing ligand)
Upon ligand engagement, BCMA activates intracellular signaling pathways that promote plasma cell proliferation and resistance to apoptosis.
Major downstream pathways include:
NF-κB signaling pathway
PI3K–AKT signaling pathway
MAPK signaling cascade
These pathways support the survival and expansion of myeloma cells within the bone marrow microenvironment.
From a therapeutic perspective, BCMA represents an ideal immunotherapy target because it exhibits:
High expression in multiple myeloma cells
Minimal expression in non-plasma cell tissues
Essential role in plasma cell survival signaling
These properties allow selective targeting of malignant plasma cells while limiting off-target toxicity.
CD3ε: The T-Cell Engagement Domain
The second functional arm of Teclistamab binds CD3ε, a critical component of the T-cell receptor (TCR) complex.
The CD3 complex consists of several subunits:
CD3γ
CD3δ
CD3ε
CD3ζ homodimer
The CD3ζ chains contain immunoreceptor tyrosine-based activation motifs (ITAMs) that initiate intracellular signaling following T-cell receptor engagement.
When Teclistamab binds CD3ε:
Polyclonal T cells are recruited to tumor cells
T-cell receptor clustering occurs
Intracellular signaling pathways are activated
Importantly, this process occurs independently of antigen presentation, allowing T cells to eliminate tumor cells even when major histocompatibility complex (MHC) expression is reduced or absent.
Fc Engineering and Pharmacologic Design
Teclistamab contains a modified IgG4 Fc region designed to optimize pharmacokinetic and safety profiles.
Key Fc modifications provide:
Reduced binding to Fcγ receptors
Decreased antibody-dependent cellular cytotoxicity (ADCC)
Reduced complement activation
Extended serum half-life (~3–4 days)
These features enable intermittent subcutaneous dosing rather than continuous intravenous infusion.
Mechanism of Action of Teclistamab
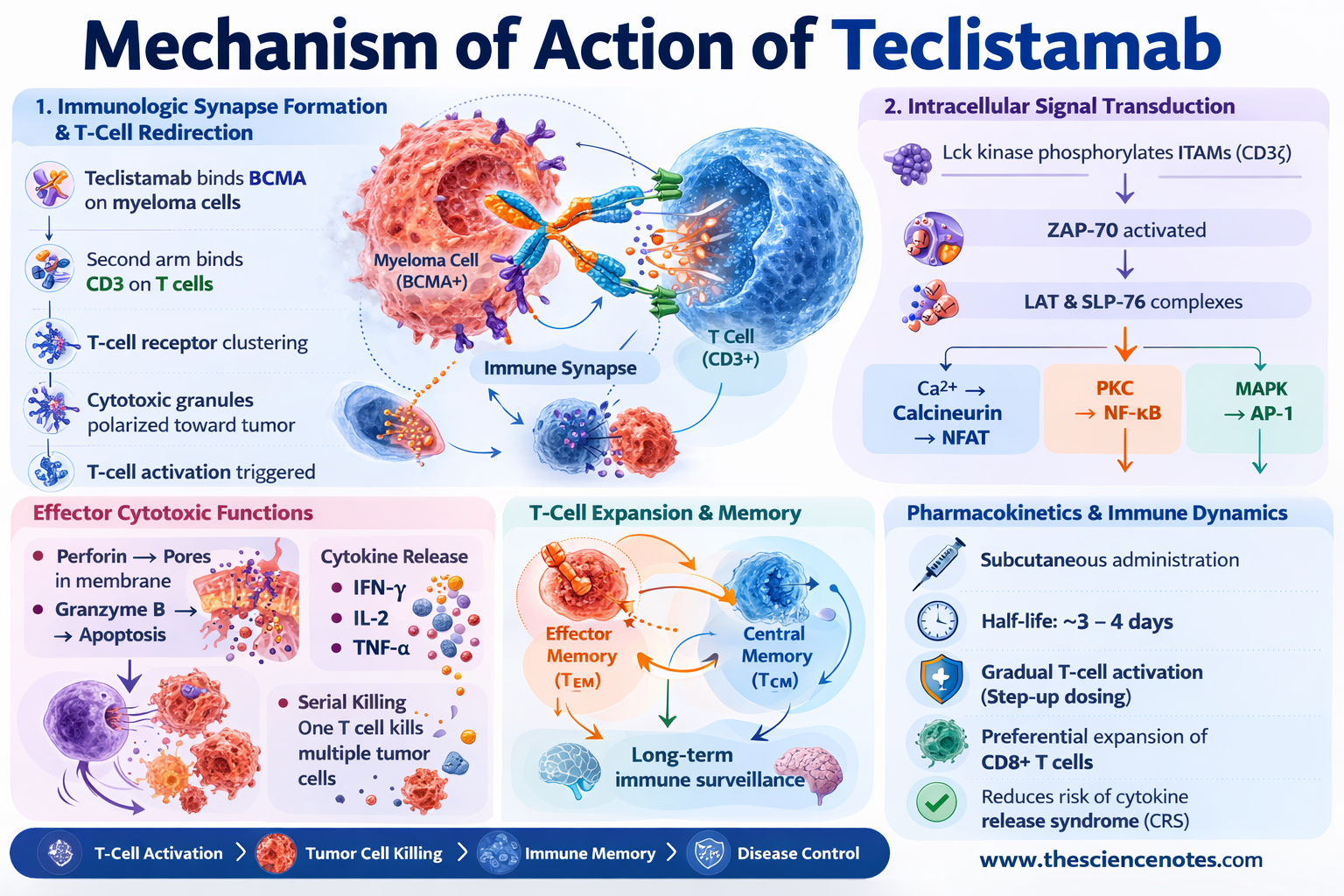
1. Immunologic Synapse Formation and T-Cell Redirection
Teclistamab functions by physically linking CD3-positive T cells to BCMA-expressing myeloma cells, thereby forming a functional cytotoxic immune synapse.
The process involves several sequential steps:
Teclistamab binds BCMA on malignant plasma cells.
The second binding arm engages CD3 on T cells.
Close cellular proximity induces T-cell receptor clustering.
Cytotoxic granules are polarized toward the tumor cell interface.
This artificial synapse mimics physiological immune cell interactions and triggers T-cell activation.
Intracellular Signal Transduction
Following CD3 engagement, a cascade of intracellular signaling events occurs:
Lck kinase phosphorylates ITAMs on CD3ζ chains
ZAP-70 is recruited and activated
Adaptor proteins including LAT and SLP-76 assemble signaling complexes
Downstream signaling pathways are subsequently activated:
Calcium–calcineurin signaling → NFAT activation
Protein kinase C signaling → NF-κB activation
MAP kinase cascade → AP-1 transcriptional activation
Together, these transcriptional programs drive T-cell activation, proliferation, and cytotoxic activity.
Effector Cytotoxic Functions
Activated T cells eliminate tumor cells through multiple mechanisms:
Perforin–Granzyme Cytotoxicity
Perforin forms pores in tumor cell membranes, allowing granzyme B to enter and trigger apoptosis.
Cytokine Release
Activated T cells release inflammatory cytokines such as:
IFN-γ
IL-2
TNF-α
These cytokines enhance immune activation and recruit additional immune cells.
Serial Killing
A single activated T cell can disengage and sequentially destroy multiple tumor cells.
2. T-Cell Expansion and Immune Memory
In addition to immediate cytotoxic effects, Teclistamab promotes expansion of T-cell populations including:
Effector memory T cells (T_EM)
Central memory T cells (T_CM)
These memory populations may contribute to long-term immune surveillance and sustained disease control.
Pharmacokinetics and Immune Dynamics
Teclistamab demonstrates favorable pharmacokinetic properties due to its IgG-based structure.
Important characteristics include:
Subcutaneous administration
Half-life of approximately 3–4 days
Gradual T-cell activation with step-up dosing
Preferential expansion of CD8+ cytotoxic T cells
Step-up dosing protocols are implemented to reduce the risk of cytokine release syndrome.
Clinical Efficacy of Teclistamab in Multiple Myeloma
MajesTEC-1 Clinical Trial
The MajesTEC-1 phase I/II trial evaluated Teclistamab in patients with heavily pretreated relapsed or refractory multiple myeloma.
Participants had previously received multiple therapy classes including:
Proteasome inhibitors
Immunomodulatory drugs
Anti-CD38 monoclonal antibodies
Key clinical outcomes included:
Overall response rate (ORR): ~63%
Complete response or better: ~39%
Median duration of response: ~18 months
These results demonstrate strong activity in patients with otherwise limited treatment options.
Adverse Events and Toxicity
Despite its therapeutic efficacy, Teclistamab is associated with several immune-related adverse effects.
Cytokine Release Syndrome (CRS)
CRS is the most common toxicity and occurs due to rapid immune activation.
Symptoms may include:
Fever
Hypotension
Hypoxia
Elevated inflammatory cytokines
Most cases are grade 1–2 and manageable with supportive therapy or IL-6 blockade.
Infections
Teclistamab may reduce normal plasma cells, leading to:
Hypogammaglobulinemia
Increased susceptibility to bacterial and viral infections
Patients may require immunoglobulin replacement therapy.
Neurotoxicity
Immune effector cell–associated neurotoxicity syndrome (ICANS) may occur, though less frequently than with CAR-T therapy.
Symptoms can include:
Confusion
Aphasia
Seizures (rare)
Mechanisms of Resistance to Teclistamab
1. BCMA Antigen Loss or Downregulation
Tumor cells may evade immune targeting by reducing BCMA expression through:
Genetic mutations
Transcriptional suppression
Shedding of soluble BCMA
Loss of surface antigen reduces antibody binding and T-cell recruitment.
2. T-Cell Exhaustion
Chronic immune stimulation may lead to dysfunctional T cells characterized by:
Upregulation of inhibitory receptors (PD-1, TIM-3, LAG-3)
Reduced cytokine production
Decreased cytotoxic capacity
3. Immunosuppressive Tumor Microenvironment
The bone marrow microenvironment of multiple myeloma contains several suppressive immune components:
Regulatory T cells (Tregs)
Myeloid-derived suppressor cells (MDSCs)
Immunosuppressive cytokines such as IL-10 and TGF-β
These factors impair effective T-cell responses.
Strategies to Overcome Teclistamab Resistance
Several therapeutic strategies are under investigation.
Dual-Target Bispecific Antibodies
Targeting additional plasma cell antigens may reduce antigen escape.
Examples include:
GPRC5D
FcRH5
Immune Checkpoint Inhibition
Combining Teclistamab with checkpoint inhibitors may restore exhausted T cells.
Potential combinations include:
Anti-PD-1 antibodies
Anti-PD-L1 therapies
Enhancing T-Cell Fitness
Strategies to improve T-cell persistence include:
Cytokine therapy (IL-7, IL-15)
Combination with immunomodulatory drugs. More Teclistamab plus Daratumumab in Relapsed or Refractory Multiple Myeloma | New England Journal of Medicine
Adoptive cellular therapies
Comparison With CAR-T Cell Therapy
Both Teclistamab and CAR-T therapies target BCMA but differ in their approach.
Teclistamab
Off-the-shelf antibody therapy
No genetic modification required
Subcutaneous administration
CAR-T Therapy
Requires genetic engineering of patient T cells
Personalized manufacturing process
Potentially longer-lasting responses
Each therapy offers unique advantages depending on clinical circumstances.
Conclusion
Teclistamab represents a major advancement in the immunotherapy of multiple myeloma by enabling potent BCMA-directed T-cell redirection. Its bispecific antibody design allows effective tumor killing independent of antigen presentation while maintaining favorable pharmacokinetic properties. Although challenges such as antigen escape, T-cell exhaustion, and immunosuppressive microenvironments remain, ongoing research into combination therapies and next-generation bispecific antibodies holds significant promise. Continued integration of molecular biology, immunology, and clinical innovation will be essential for optimizing Teclistamab-based treatments and achieving durable remissions in multiple myeloma.
Frequently Asked Questions (FAQ)
Q1. What is Teclistamab?
Teclistamab is a bispecific antibody that targets BCMA on multiple myeloma cells and CD3 on T cells, enabling immune-mediated tumor killing.
Q2. Why is BCMA an important target in multiple myeloma?
BCMA is highly expressed on malignant plasma cells and plays a crucial role in plasma cell survival signaling.
Q3. What are the main side effects of Teclistamab?
Common side effects include cytokine release syndrome, infections, and occasional neurotoxicity.
Q4. How does Teclistamab differ from CAR-T therapy?
Teclistamab redirects existing T cells using an antibody, whereas CAR-T therapy involves genetically modifying patient T cells.
Q5. What causes resistance to Teclistamab?
Resistance may arise from BCMA antigen loss, T-cell exhaustion, or immunosuppressive factors within the tumor microenvironment.