Endometriosis is a complex, often misunderstood chronic inflammatory disease that affects millions of women and individuals assigned female at birth globally. Despite its prevalence—affecting approximately 10% of women of reproductive age—it often takes years to receive an accurate diagnosis.
In this comprehensive guide, we will explore the nuances of endometriosis, its impact on fertility, and the latest medical advancements in managing its symptoms.
What is Endometriosis?
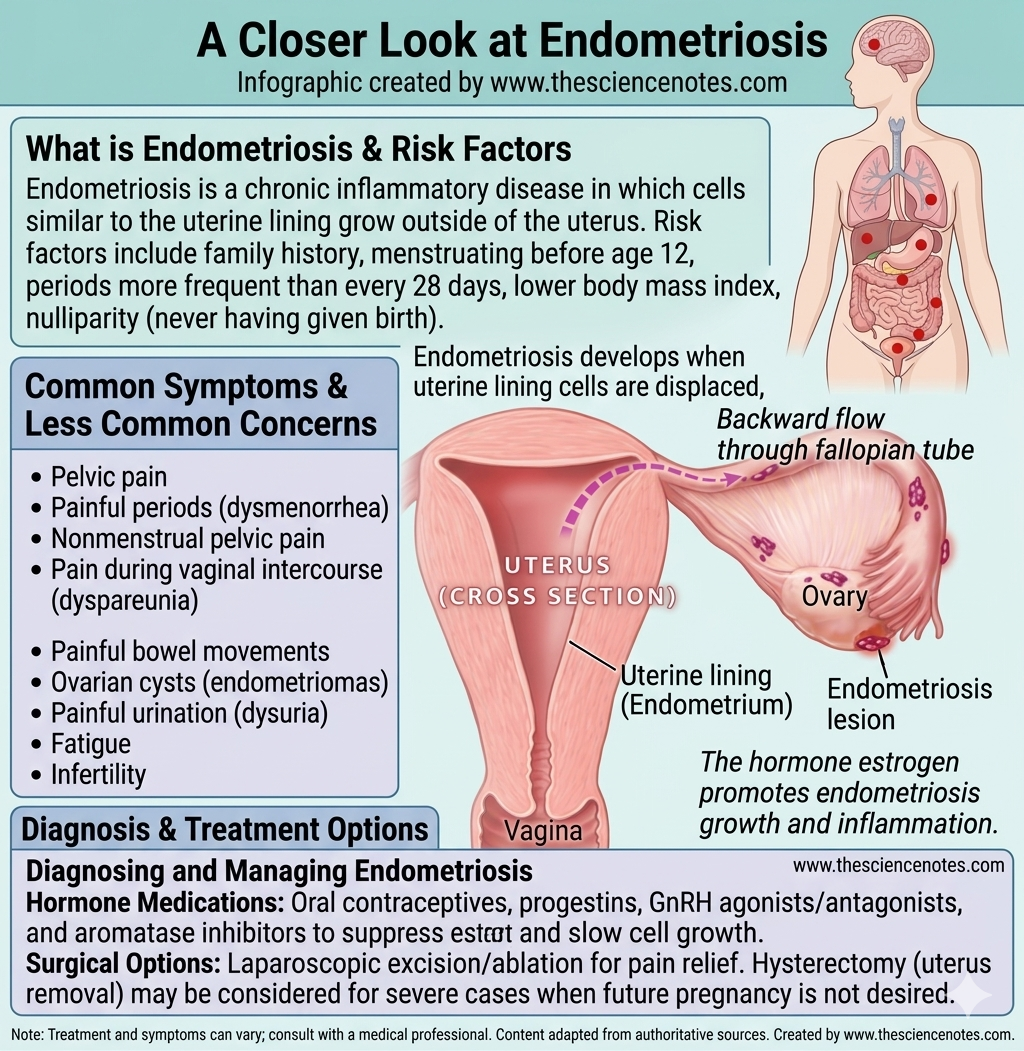
Endometriosis occurs when tissue similar to the lining of the uterus (the endometrium) begins to grow in places where it doesn’t belong. While the endometrium is designed to thicken and shed during a menstrual cycle, endometriosis “lesions” or “growths” outside the uterus have no way to exit the body.
Common Areas Where Endometriosis Grows:
Ovaries: Where it can form “chocolate cysts” known as endometriomas.
Fallopian Tubes: Which can lead to scarring and fertility issues.
Outer Surface of the Uterus: And the ligaments that support it.
Bowel and Bladder: Leading to digestive or urinary complications.
Remote Sites: In rare cases, it has been found in the lungs, skin, and even the brain.
How Does Endometriosis Develop?
The exact cause of endometriosis remains one of the greatest mysteries in modern gynecology. However, several leading theories explain how these rogue cells migrate and thrive:
Retrograde Menstruation: This is the most widely accepted theory. It suggests that during a period, menstrual blood containing endometrial cells flows backward through the fallopian tubes into the pelvic cavity instead of leaving the body.
Cellular Transformation: Some researchers believe that hormones or immune factors transform cells outside the uterus into endometrial-like cells.
Surgical Scar Implantation: Endometrial cells may attach to surgical incisions, such as those from a C-section or hysterectomy.
Lymphatic or Blood Stream Spread: Similar to how cancer cells move, endometrial cells may travel through the blood or lymphatic system to distant organs like the lungs.
Recognizing the Signs and Symptoms
The hallmark of endometriosis is pain, but the intensity of the pain does not always correlate with the severity of the disease. A person with “mild” endometriosis may experience debilitating pain, while someone with “severe” Stage IV disease may have no symptoms at all.
Key Symptoms to Watch For:
Dysmenorrhea (Painful Periods): Pelvic pain and cramping that may begin before and extend several days into a menstrual period.
Chronic Pelvic Pain: Persistent lower back and pelvic pain that isn’t limited to the menstrual cycle.
Dyspareunia: Pain during or after sexual intercourse.
Painful Bowel Movements or Urination: Most common during your period.
Excessive Bleeding: Occasionally experiencing heavy menstrual periods or bleeding between periods (intermenstrual bleeding).
Infertility: For many, endometriosis is first diagnosed during an evaluation for infertility.
Note: Digestive issues like bloating (often called “Endo Belly”), nausea, and fatigue are also frequently reported, sometimes leading to a misdiagnosis of Irritable Bowel Syndrome (IBS).
Risk Factors: Who is Most at Risk?
While any person who menstruates can develop endometriosis, certain factors increase the likelihood:
Family History: Having a mother, sister, or aunt with the condition.
Menstrual History: Starting your period before age 12, or having cycles shorter than 27 days.
Body Mass Index (BMI): Interestingly, a lower BMI is often linked to a higher risk of endometriosis.
Nulliparity: Never having given birth.
High Estrogen Levels: Endometriosis is an estrogen-dependent condition.
The Path to Diagnosis: Why is it Difficult?
On average, it takes 7 to 10 years for a patient to receive a formal diagnosis of endometriosis. This is often due to the normalization of “period pain” in society and the fact that symptoms overlap with other conditions.
Diagnostic Tools:
Pelvic Exam: A doctor manually feels for large cysts or scars.
Ultrasound: Useful for identifying endometriomas (cysts on the ovaries).
MRI: Provides detailed images of soft tissues to help surgeons plan for excision.
Laparoscopy: This is the gold standard. A surgeon performs a minimally invasive procedure to look inside the abdomen and take a biopsy of the tissue.
Treatment Options: Managing a Chronic Condition
While there is currently no cure for endometriosis, treatment focuses on managing pain and improving fertility.
1. Hormone Therapy
Hormones are used to lower estrogen levels or stop the menstrual cycle, which prevents the growths from bleeding and causing inflammation.
Hormonal Contraceptives: Birth control pills, patches, and vaginal rings.
GnRH Agonists and Antagonists: These drugs put the body into a “temporary menopause” state to shrink lesions.
Progestin-Only Therapy: Such as the Depo-Provera shot or a hormonal IUD (Mirena).
2. Pain Management
NSAIDs: Over-the-counter anti-inflammatories like Ibuprofen or Naproxen are often the first line of defense.
Neuropathic Pain Meds: For chronic pelvic pain that involves nerve sensitivity.
3. Surgical Intervention
Excision Surgery: The surgeon cuts out the endometriosis lesions. This is generally preferred over “ablation” (burning the tissue), as it has a lower recurrence rate.
Hysterectomy: In severe cases where other treatments have failed, removing the uterus (and sometimes the ovaries) may be considered, though this is not a guaranteed cure for the pain.
4. Lifestyle and Complementary Medicine
Managing inflammation through lifestyle can provide significant relief:
Anti-Inflammatory Diet: Reducing processed sugars, caffeine, and alcohol.
Regular Exercise: Helps lower circulating estrogen and releases endorphins (natural painkillers).
Physical Therapy: Pelvic floor physical therapy is highly effective for addressing the muscle tension and “guarding” caused by chronic pain.
Endometriosis and Fertility
Infertility is a major concern, affecting nearly 50% of women with the condition. Endometriosis can affect fertility by:
Distorting Anatomy: Scar tissue and adhesions can block or twist the fallopian tubes.
Egg Quality: Inflammation may affect the quality of eggs or the environment in the ovaries.
Implantation Issues: The uterine lining may be less receptive to an embryo.
The Good News: Many people with endometriosis go on to have healthy pregnancies. Laparoscopic surgery to remove lesions and Assisted Reproductive Technologies (ART) like IVF are highly successful options for those struggling to conceive.
Associated Health Conditions
Research suggests that endometriosis is not an isolated pelvic issue but a systemic inflammatory condition. It has been linked to:
Autoimmune Diseases: Such as Lupus, Multiple Sclerosis, and Rheumatoid Arthritis.
Chronic Fatigue Syndrome and Fibromyalgia.
Certain Cancers: A slightly increased risk of epithelial ovarian cancer.
Summary: Living Well with Endometriosis
Endometriosis is a life-altering condition, but it does not have to define your life. Early intervention, a multidisciplinary medical team (including a GYN specialist, a pelvic PT, and perhaps a nutritionist), and a strong support system are the keys to managing this chronic journey.
If you suspect you have endometriosis, trust your body. Pain that interferes with your daily life is not “normal.” Advocate for yourself, seek a specialist, and explore the treatment path that aligns with your personal health goals.
FAQs about Endometriosis
Can endometriosis be prevented? No, it cannot be prevented, but you can reduce your risk by maintaining lower estrogen levels through regular exercise and limited alcohol/caffeine intake.
Does endometriosis go away after menopause? For many, symptoms improve as estrogen levels drop naturally. However, if you use Hormone Replacement Therapy (HRT), symptoms may persist.
Is endometriosis a type of cancer? No, endometriosis growths are benign (non-cancerous), though they can behave aggressively by invading nearby organs.