Amoebiasis remains one of the most significant parasitic challenges in global health. Caused by the protozoan parasite Entamoeba histolytica, this infection ranges from asymptomatic colonization to severe invasive disease. Understanding the biology, life cycle, and pathology of this organism is essential for effective diagnosis and prevention.
1. Scientific Classification and Taxonomy
To understand E. histolytica, we must first look at its place in the biological world. It belongs to a group of organisms characterized by their fluid shapes and “creeping” movement.
Phylum: Sarcomastigophora
Sub-phylum: Sarcodina
Class: Lobosea
Genus: Entamoeba
Species: histolytica
While several species within the Entamoeba genus colonize the human gut (such as E. coli or E. dispar), Entamoeba histolytica is the primary pathogen. It is a microscopic organism, roughly 60µm in size, capable of causing extensive tissue destruction—hence the name “histolytica” (histo = tissue, lytica = dissolving).
2. Habitat and Geographical Distribution
The primary “home” of E. histolytica is the lumen of the colon or the large intestine of the human host. However, its prevalence is not uniform across the globe.
Where is it most common?
Amoebiasis is highly endemic in regions with limited modern sanitation systems. This includes:
Mexico and Central America
Western South America
South Asia
Western and Southern Africa
Environmental Factors
While the parasite thrives in warmer climates, this is less about the temperature itself and more about hygiene infrastructure. In warm, moist conditions, the hardy cysts of the parasite can survive for extended periods outside the host, increasing the window for transmission through contaminated food and water.
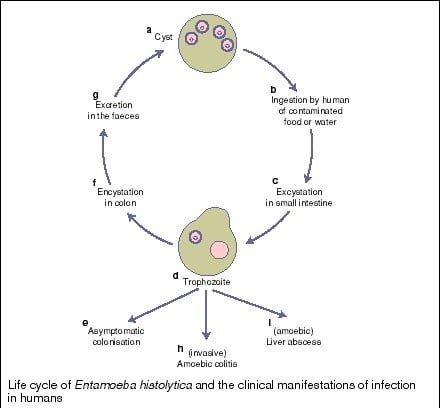
3. The Life Cycle of E. histolytica
The life cycle is relatively straightforward but highly effective at ensuring the parasite’s survival. It exists in two main forms: the Cyst (the infectious, dormant stage) and the Trophozoite (the active, disease-causing stage).
Stage 1: Ingestion
The cycle begins when a human consumes mature quadrinucleate cysts. This usually happens via “fecal-oral” transmission—consuming food or water contaminated with infected feces or through poor hand hygiene.
Stage 2: Excystation
Once the cysts pass through the stomach, the acidic environment triggers excystation in the small intestine. This releases the active trophozoites, which then migrate to the large intestine.
Stage 3: Multiplication and Invasion
In the large intestine, trophozoites multiply by binary fission. From here, one of three paths is taken:
Non-invasive: Trophozoites stay in the lumen, feed on bacteria, and eventually turn back into cysts (encystation) to be passed in stool.
Intestinal Disease: Trophozoites invade the intestinal mucosa.
Extraintestinal Disease: Trophozoites enter the bloodstream and travel to organs like the liver, lungs, or brain.
Survival Outside the Host
Cysts are protected by a thick wall, allowing them to survive for weeks in the environment. Trophozoites, however, are fragile. If passed in stool, they die quickly; even if swallowed, they cannot survive the stomach’s gastric acid. Therefore, cysts are the primary vehicles of transmission.
4. Clinical Manifestations of Amoebiasis
The pathology of E. histolytica is driven by histolysin, a proteolytic enzyme the parasite secretes to dissolve human tissue. After an incubation period of 1 to 4 weeks, the infection manifests in one of three ways:
A. Asymptomatic Infection
The majority of infected individuals are “carriers.” They harbor the parasite and pass infectious cysts in their stool but do not experience symptoms. These individuals are crucial to the spread of the disease in communities.
B. Intestinal Amoebiasis
When the parasite invades the colon lining, it creates characteristic flask-shaped ulcers. Symptoms include:
Bloody diarrhea (Amoebic dysentery)
Severe abdominal pain and cramping
Mucus in the stool
C. Extra-intestinal Amoebiasis
If the trophozoites breach the intestinal wall and enter the circulatory system, they can cause abscesses in distant organs.
Liver: The most common site, leading to amoebic hepatitis or liver abscesses.
Lungs & Brain: Less common but life-threatening infections.
Appendicitis: Occasionally, the parasite can cause inflammation of the appendix.
5. Laboratory Diagnosis
Accurate diagnosis is vital because E. histolytica looks identical to the non-pathogenic E. dispar under a basic microscope.
Stool Examination: Doctors look for cysts (in formed stool) or trophozoites (in watery stool). Because the parasite isn’t shed constantly, a minimum of three separate stool samples is usually required.
Macroscopy: Observation of stool for the presence of blood and mucus.
Serologic Tests: Blood tests (ELISA, IHA, IFA) detect antibodies against the parasite.
Pus Aspiration: If a liver abscess is suspected, the aspirated pus often has a distinct “anchovy sauce” appearance (reddish-brown).
PCR: The most definitive way to distinguish E. histolytica from non-pathogenic species.
6. Treatment and Prevention
Treatment typically requires a multi-pronged approach to ensure both the active parasites and the dormant cysts are eliminated.
Medical Treatment
Tissue-active agents: Metronidazole or Tinidazole (to kill trophozoites in tissues).
Luminal agents: Diloxanide (to clear cysts from the gut).
Chloroquine: Sometimes used specifically for liver-based infections.
Prophylaxis (Prevention)
Personal Prophylaxis:
Wash hands with soap and hot water for at least 10 seconds after using the toilet or changing diapers.
Maintain strict bathroom cleanliness.
Avoid sharing personal items like towels.
Community Prophylaxis:
Water Safety: Boil water or use iodine tablets in endemic areas.
Food Safety: Avoid raw vegetables fertilized with “night soil” (human feces) and be cautious of street foods where shared containers are used.
Entamoeba histolytica is a formidable parasite, but through a combination of modern medicine and rigorous hygiene, its impact can be mitigated. Whether you are traveling to an endemic area or studying microbiology, the key to staying safe is understanding the invisible life cycle occurring beneath the surface.
Understanding the Life Cycle Stages
The parasite essentially flips between a “survival mode” and an “attack mode” depending on its environment.
The Cyst (Survival Mode): This is the infectious stage. It is a hardy, quadrinucleate (four-nuclei) sphere that can survive outside the body. It is resistant to the chlorine levels found in many municipal water systems, which is why boiling water is often necessary in endemic areas.
The Trophozoite (Attack Mode): Once the cyst reaches the alkaline environment of the small intestine, it “hatches” into trophozoites. These are motile, actively feeding, and reproduce via binary fission. They are responsible for the actual tissue destruction using histolysin.
Key Diagnostic Visuals
When diagnosing a patient, medical professionals look for specific “red flags” in laboratory samples:
Flask-Shaped Ulcers: In a colonoscopy, the damage doesn’t look like a standard scrape; it looks like a narrow-necked bottle or flask because the parasite eats horizontally once it gets beneath the surface layer.
Anchovy Sauce Pus: If an abscess is drained from the liver, the fluid has a very distinct reddish-brown color and thick consistency, which is pathognomonic (specifically characteristic) for amoebic liver abscesses.
Quick Prevention Checklist
Heat: Cysts are killed by temperatures above 55°C (131°F).
Hygiene: Proper sewage disposal is the only way to break the cycle at a community level.
Peel it, Cook it, or Forget it: A classic rule for travelers in endemic regions to avoid contaminated raw produce.