The period that begins after 8th week following conception and ends in delivery is termed as fetal period. Fetus growth and changes in physiological system in described in this article.
How to determine the fetal age?
Age of fetus is determined in term of gestational age from first day of last menstrual period.
To determine age of fetus, crown-rump length is most accurate. It is measured via ultrasonography in first trimester from vertex to the coccyx. Gestational age can be determined by adding 42 days in crown-rump length with an error of 2.1 days in the first trimester.
Growth of fetus:
In the first half of the pregnancy, growth of fetus is controlled by genetic factors and in the second half of the pregnancy, growth of fetus is controlled by environmental factors.
What are the physiological factors that influence the growth of fetus?
- European babies are heavier than Indians
- Male fetus weigh more than female fetus
- Pre pregnant weight, weight gain during pregnancy, education of pregnant female.
- Babies born to taller and heavier mother will be heavy
- In second pregnancy weight of the baby is more compared to first.
- Major determinant of fetal growth is utero placental blood flow, trans placental glucose and fetal insulin.
Physiological changes during fetal period
- 2/3rd of total calcium, 3/5th of total proteins and 4/5th of total iron are drained from mother during last 3 months of pregnancy.
Fetal blood :
- Hematopoiesis is demonstrated by 14th day in yolk sac, by 10th week in liver.
- During first half, hemoglobin is fetal type, but from 24weeks onward, adult type of hemoglobin appears and at term about 75-80% of total hemoglobin is of fetal type.
- Rh factor is determined from 38 days after conception.
- Life span of fetal RBC is 2/3rd of adult RBC (80 days).
- Passive immunity to fetus is provided from 12th week onwards.
Fetal Respiratory system:
- In early months lungs are solid.
- At 24th week, lung surfactants appear secreted by type-2 alveolar cells.
- L:S ratio of 2:1 in liquor amnii suggest full maturity of fetal lungs.
- Breathing movement is seen by 11th weeks but are irregular until 20th week.
Fetal Cardiovascular system :
- Human heart starts beating during the 4th week after fertilization.
- Rate of contraction is about 65 beats/minute which increases steadily to about beats/minute immediately before birth.
Fetal Endocrinology:
- Growth hormone, ACTH, prolactin, TSH and gonadotropin are produced as early as 10th week.
- By 12th week vasopressor and oxytocic activity are demonstrated.
- Thyroxine is synthesized by 11th week.
- Insulin is secreted by 12th week and glucagon by 8th week.
Fetal Gastrointestinal tract:
- Fetus swallows amniotic fluid as early as 10-12 weeks.
- From 20th week and at term meconium appears.
Fetal Urinary system:
- Nephrons become active and start secreting urine by end of the first trimester.
- Urine production rises to 650 ml/day near term.
Fetal Central nervous system:
- Most of the reflexes are present by the 3rd to 4th months of pregnancy.
- Development of sub cortical brain structures occurs from 12-22 weeks.
- Myelination of the ventral roots of the cerebrospinal nerves and brainstem begins at approximately 6 months but most myelination occurs after birth.
Fetal Skin:
- Lanugo hair appears at 16th week and almost completely disappears at near term.
- At 12th week sebaceous gland appear.
Fetal circulation
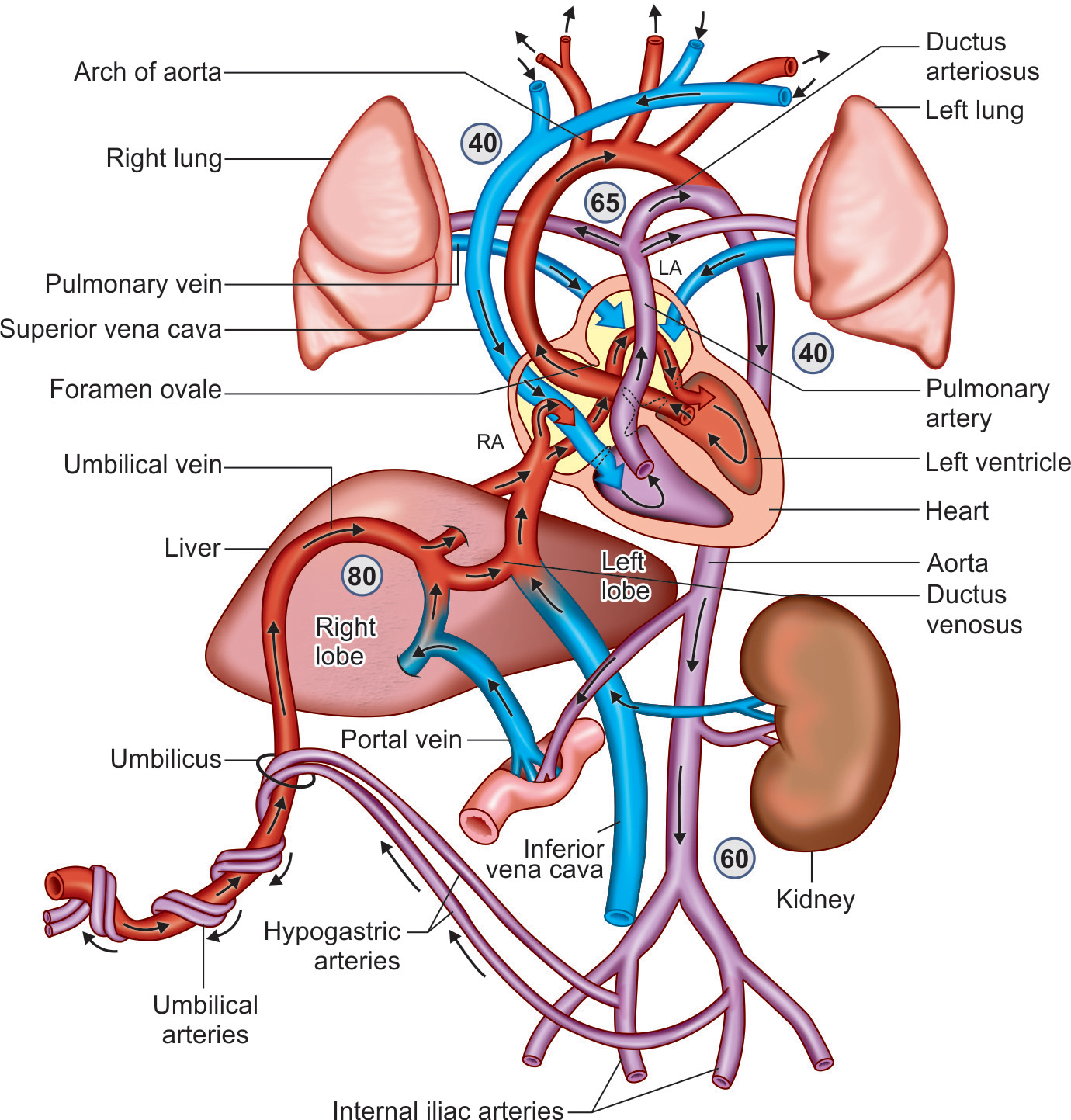
Figure 1: Fetal circulation
- In the fetal period, source of oxygenated blood is not the lung. Oxygenated blood is supplied through placenta.
- Oxygenated blood comes to fetus through umbilical vein, which joins the left branch of the portal vein. Greater part of blood passes directly to the inferior venecava through ductus venosus, and small portion of blood passes through the substance of liver to the inferior venecava.
- Oxygen rich blood is carried by inferior venecava to the right atrium and is directed towards the foramen ovale. Most of it passes through the foramen ovale into left atrium and rest of it gets mixed up with the blood from superior venecava in the right atrium, and passes into the right ventricle.
- From the right ventricle, the blood enters the pulmonary trunk and small portion of this reaches to the lungs and then to the left atrium. Most of the blood is diverted into the aorta through ductus arteriosus.
- From the left atrium, which has received blood from right atrium and lungs, blood passes into the left ventricle and then into the aorta. Oxygen rich blood passes into carotid and subclavian arteries to the brain and rest of it gets mixed with poorly oxygenated blood from ductus arteriosus. Thus the parts of body supplied by branches of aorta distal to the junction with ductus arteriosus receive blood with moderate oxygen content.
- Much of the blood of the aorta is carried by umbilical arteries to the placenta where it is again oxygenated and returned to the heart.
Changes in fetal circulation after birth
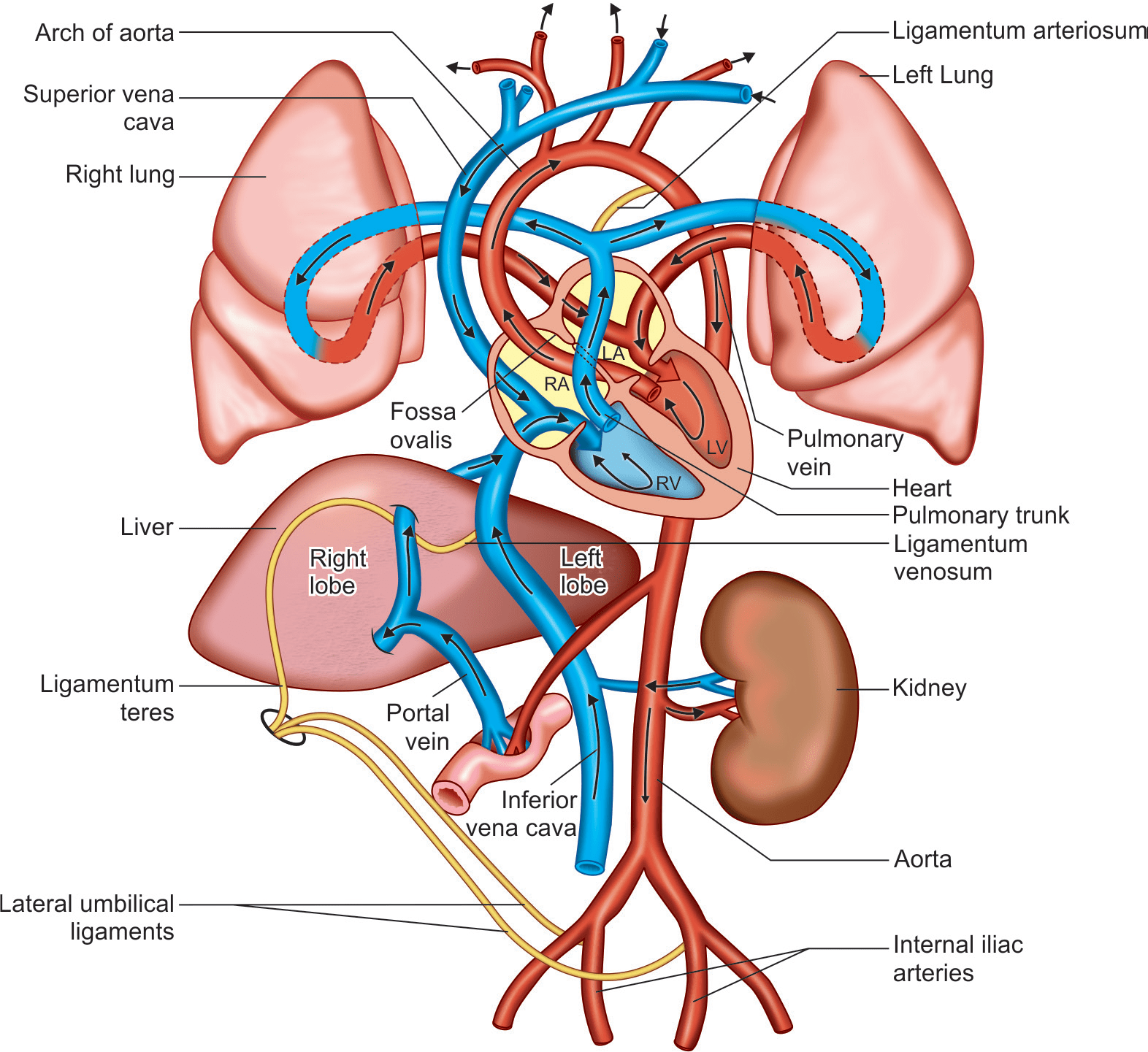
Figure 2: Changes in fetal circulation after birth
- Umbilical arteries contracts immediately after birth and occludes their lumen.Actual obliteration takes about 2-3 months. After obliteration of umbilical arteries it forms medial umbilical ligaments.
- Umbilical vein takes a little more time than arteries to obliterate allowing few extra volume of blood (80-100 ml) to be received by the fetus from placenta. After obliteration of umbilical vein it forms ligamentum teres.
- Ductus venosus also collapse and form ligamentum venosum.
- Functional closure of ductus arteriosus may occur soon after the establishment of pulmonary circulation, the anatomical obliteration takes about 1-3 months. After obliteration of ductus arteriosus, ligamentum arteriosum is formed.
- Foramen ovale closes functionally soon after birth but anatomically in about 1 year time.
References:
- Guyton and Hall Textbook of Physiology; 13th Edition
- DC Dutta’s Textbook of OBSTETRICS; 9th Edition
- https://pubmed.ncbi.nlm.nih.gov/7036747/
- https://www.ajog.org/article/0002-9378(95)90478-6/fulltext